Comforting speeches won’t cure Alzheimer’s
Alzheimer’s patients deserve leaders whose actions are as committed as their promises.

Alzheimer’s patients deserve leaders whose actions are as committed as their promises.
Alzheimer’s patients deserve leaders whose actions are as committed as their promises.
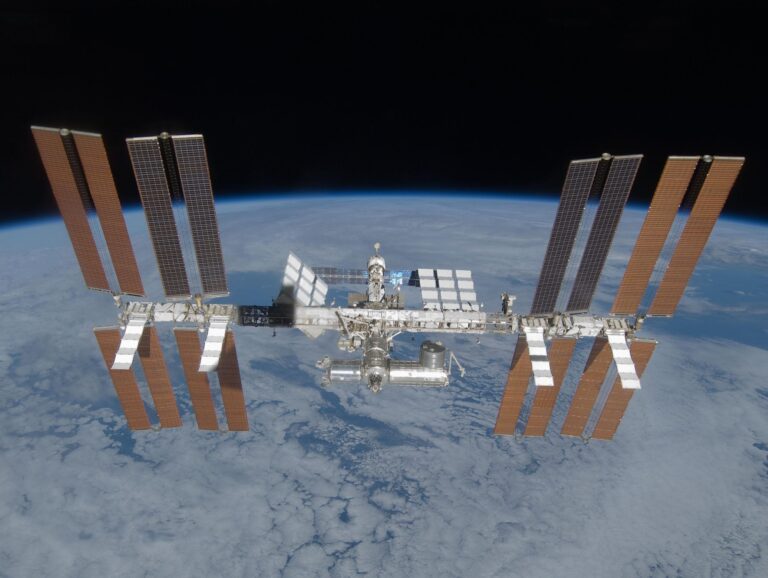
What will happen to research conducted in space when the International Space Station ends in 2030?

Long-term care coverage is not a one-size-fits-all solution.

Last year, I joined an exclusive group – Americans who have price shopped for their health care. And it wasn’t great…

Dual-eligible patients face some of the largest gaps in SUD treatment. The problem isn’t a lack of solutions.

Gene therapies can cure once-incurable diseases, but without payment reform, America’s insurance system will keep them out of reach for many patients.


A new FDA program promises ultra-fast drug approvals for “national priorities,” raising questions about politics, science, and public trust.

Five years after hospital price transparency, costs keep rising – showing that publishing prices alone can’t lower spending without enforcement and real competition.

Medicare’s hospital trust fund will be insolvent by 2033. Without change, older adults and hospitals face painful, automatic cuts to inpatient care.

Massachusetts has a chance to lead on state policy around Alzheimer’s and dementia in 2026, if lawmakers choose to prioritize it.

Medicaid retroactive coverage changes shift costs to patients, but hospitals can cushion the impact using 340B funds
A more useful definition of dementia-friendliness must center on state policy.